Sinusitis, as the name suggests, is an inflammation of the sinuses. Horses suffering with sinusitis can be frustrating for owners to deal with for a couple of reasons – one, that they often present with a nasal discharge that is persistent, smelly, and unsightly, and two, they can be difficult to resolve, often requiring surgical involvement to recover fully.
Sinuses are air-filled cavities within the skull that connect either directly or indirectly with the nasal passages, allowing an interchange of air, fluid, and infectious agents between the two. The horse has six paired sinuses in the skull, these being the maxillary sinuses, the frontal sinuses, the sphenopalatine sinuses, and the dorsal, middle, and ventral concha sinuses.
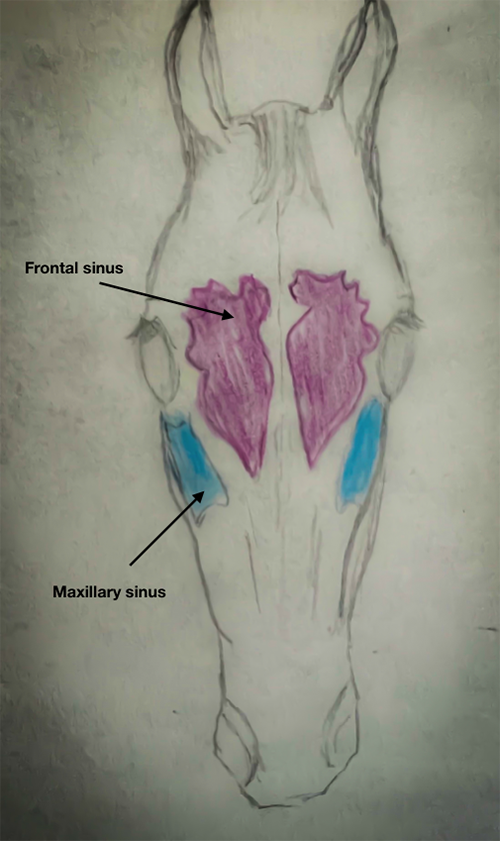
The frontal sinus is triangular-shaped and located below the skull bones that sit between the eyes and extends down to approximately midway along the facial crest. The frontal sinus communicates with the dorsal conchal sinus and can sometimes be referred to as the conchofrontal sinus. Frontal sinusitis can often occur because of trauma, as it becomes infected secondarily to the horse running directly into an object (especially trees), fracturing the front of the skull and introducing bacteria into the environment.
The maxillary sinus is the largest of the sinuses and is divided into rostral and caudal parts by a thin septum (bony wall). The caudal part of the maxillary sinus is the larger and communicates with the sphenopalatine sinus, the middle conchal sinus and the frontal sinus. In foals, the maxillary sinus is full of developing teeth, and by the time a horse has reached 5 to 6 years old, the sinus is filled with the embedded parts of teeth. As the horse ages the teeth move down from the sinus into the mouth to ensure enough tooth is present to compensate for the wear that occurs with grazing and chewing. By the time the horse becomes “old”, the maxillary sinus becomes more air filled and eventually all the teeth that occupied the region are lost.
The rostral maxillary sinus is the most common sinus affected with sinusitis, with a recent CT study showing that almost 95% of sinusitis cases studied involved this site. The next most common site is the ventral conchal sinus, with the sphenopalatine sinus being the least affected. This is because the rostral maxillary sinus and the ventral conchal sinus are the two lowest sinus cavities when the horse is grazing (has its head down) and therefore drain less well than the sinus cavities at the top (the effect of gravity).
PRIMARY & SECONDARY
Sinusitis can be primary or secondary in nature. Primary infections occur when bacteria (or occasionally fungi) gain access into the sinus via the upper airways causing an infection. Secondary infections occur as an extension of an infection in another structure, predominantly the teeth roots, or in conjunction with a cyst, tumour, facial bone fracture or progressive ethmoid haematoma. Secondary infections are usually more difficult to treat, as they will not recover until the underlying cause is identified and treated. Horses with Pituitary Pars Intermedia Dysfunction (PPID), also called Cushing’s, are also prone to sinus infections because the immune system is compromised, and they are often older horses that are prone to tooth root infections. The most common cause of sinusitis is one that is secondary to a dental problem, followed by primary sinus infections and then sinus cysts. Tumours, fractures, and ethmoid haematomas are far less frequent.
Clinical symptoms are similar regardless of the cause of the sinusitis and horses most often present with a persistent unilateral nasal discharge (i.e. discharge from one nostril). Often the nasal discharge resolves when the horse is treated with antibiotics, only to return once the antibiotics stop. The discharge is usually purulent and can be quite malodourous if there are diseased tooth roots or necrotic tissue caused by expanding tumours involved. Blood can be present in the discharge if tissue destruction has occurred. The facial bones may become distorted and softened if pressure within the sinus increases, as can occur with a growing tumour or cyst. If the amount of fluid/purulent mucus produced within the sinus accumulates faster than the mucus can escape out the nose, or if the openings from the sinuses become blocked, the pressure will build up in the sinus as well, causing a bulging appearance on the front of the face, just below the eyes. Other symptoms include tearing and conjunctivitis because of pressure on the nasolacrimal duct or distortion of the face.
Several diagnostic tools are available to investigate the sinuses and whether they are infected, and if infected, whether it is primary or secondary sinusitis. These include endoscopy, radiography, CT and potentially MRI (dependent of the MRI unit being available).
ENDOCOPY: An endoscope can be used initially to assess the upper airways to identify the site where the mucopurulent discharge is arising. A nasal discharge can come from the sinus, the guttural pouch, the trachea/lungs or simply be a nasal passage infection. Often with sinusitis, a stream of purulent discharge can be detected flowing down from the sinus openings that connect with the nasal passages. Sometimes there might be inspissated pus (firm dried pus) detected in the concha, indicating a chronic sinusitis. Other times, it may be difficult to see any pus coming from the sinuses and elimination of the presence of mucopurulent material in the guttural pouches or in the trachea is done using the endoscope. The scope can also be used to directly visualise the sinuses via a trephined hole into the skull.
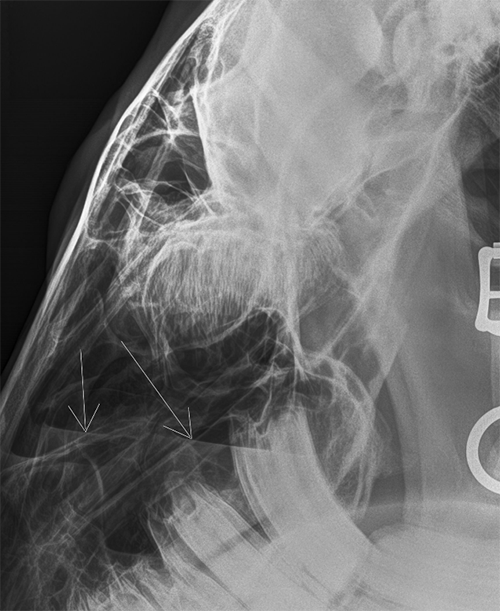
RADIOLOGY: X-rays are frequently used to diagnose sinusitis and to look for evidence of inciting causes, particularly tooth root infections or soft tissue swellings such as cysts or tumours. Fluid lines indicate fluid within the sinus and is the most common radiographic anomaly seen with sinusitis. Obliqued views are required to assess the tooth roots and identify if and what tooth is involved, as any infected tooth generally needs to be removed to resolve the sinusitis. If the initiating cause is a facial fracture, then X-rays are used both to assess the fracture and to look for fragments of bone that may be free within the sinus, causing a nidus of infection.
CT SCAN: A CT (computed tomography) scan gives superior results to both endoscopy and radiology as it offers a 3D image to assess that has much greater detail of the structures involved, including the nasal cavities and the teeth that are not as clearly identified with plain radiographs. Ideally, a standing CT is the preferred option but not all CT scans can be used this way, with some requiring the horse to undergo general anaesthesia to obtain images. The increased use of the CT scan has greatly improved the veterinary knowledge of sinusitis and led to better outcomes with treatment. CT has meant better targeting of areas to treat and has identified areas outside the sinus that require concurrent treatment to reduce the risk of treatment failure or recurrence of sinusitis once treatment has ended.
MRI: MRI (magnetic resonance imaging) has not been used as frequently as CT but does offer superior images and detail of both the bone and the soft tissues than X-rays alone. Currently, the availability of an MRI machine that can obtain head images in Australia is limited and so cannot be recommended over the use of the CT scan.

TREATMENT
Treatment for sinusitis is dependent on whether the sinusitis is primary or secondary. Primary sinusitis can be treated with systemic antibiotics alone, or with ancillary management such as feeding the horse on the ground and giving light exercise to encourage drainage. Mucolytics can help decrease the thickness/stickiness of the mucus in the sinus cavities so that it is easier for the mucus to be cleared by the small cilia in the sinus linings and therefore drain through the openings into the nasal passages and out through the nose.
If systemic antibiotic therapy doesn’t resolve the problem, then lavaging (flushing) the pus out from the sinus via a hole drilled into the sinus often works. This is a common procedure where a drill is used to trephine a hole either into the facial or maxillary sinus and daily lavages are performed until there is no more pus/discharge detected. These trephined holes quickly fill in once the flushing has stopped and usually cause the horse little if no long-term concerns.
Secondary sinusitis cases require treatment of the inciting cause as well as the treatments listed for primary sinusitis. If a tooth or teeth are infected or fractured, the offending tooth needs to be identified and the tooth removed. Similarly, cysts, tumours or ethmoid haematomas need to be removed or treated if possible, however, this may not always be possible, particularly with tumours. Some tumours found in the sinuses can be malignant and aggressive, necessitating euthanasia. Cysts can often be removed surgically, and ethmoid haematomas can be treated either surgically, with laser or via transendoscopic injections of formaldehyde into the lesion.
Horses with fractures involving the frontal sinus, may need to have bone fragments/sequestrums removed and the sinus flushed to remove foreign material to aid healing. Horses that have PPID require treatment for this (typically pergolide), and/or removal of offending teeth before a successful resolution is achieved. EQ
YOU MIGHT ALSO LIKE TO READ THE FOLLOWING BY DR MAXINE BRAIN:
Japanese Encephalitis: No Cause For Alarm – Equestrian Life, April, 2022
Hernia Learning Curve – Equestrian Life, March, 2022
Osteochondromas: Benign But Irritating – Equestrian Life, February, 2022
Don’t Forget the Water – Equestrian Life, January, 2022
Understanding Anaesthesia – Equestrian Life, December, 2021
A Quick Guide to Castration – Equestrian Life, November, 2021
Caring for Mammary Glands – Equestrian Life, October, 2021
Sepsis In Foals – Equestrian Life, September 2021
Understanding Tendon Sheath Inflammation – Equestrian Life, August 2021
The Mystery of Equine Shivers – Equestrian Life, July 2021
Heads up for the Big Chill – Equestrian Life, June 2021
The Ridden Horse Pain Ethogram – Equestrian Life, May 2021
The Benefits of Genetic Testing – Equestrian Life, April 2021
Heavy Metal Toxicities – Equestrian Life, March 2021
Euthanasia, the Toughest Decision – Equestrian Life, February 2021
How to Beat Heat Stress – Equestrian Life, January 2021
Medicinal Cannabis for Horses – Equestrian Life, December 2020
Foal Diarrhoea Part 2: Infectious Diarrhoea – Equestrian Life, November 2020
Foal Diarrhoea (Don’t Panic!) – Equestrian Life, October 2020
Urticaria Calls For Detective Work – Equestrian Life, September 2020
Winter’s Scourge, The Foot Abscess – Equestrian Life, August 2020
Core Strengthening & Balance Exercises – Equestrian Life, July 2020
The Principles of Rehabilitation – Equestrian Life, June 2020
When is Old, Too Old? – Equestrian Life, May 2020