Last month we discussed the worth of having a full cardiac examination when buying a horse. Let’s now discuss some of the types of murmurs and their significance.

Murmurs are generated by blood as it flows through the heart and into the large arteries that deliver the blood to the vital organs in the body. Any disruption to the smooth flow of blood causes turbulence and this is transmitted as a vibration through the cardiac structures, and produces an audible noise we hear with a stethoscope. Not all murmurs are pathological, meaning they aren’t all bad, and horses commonly have murmurs that are of no clinical significance.
To understand murmurs, it is good to have a basic understanding of the heart and how it functions. The heart is divided into four chambers — two atria and two ventricles. These chambers are connected by large valves that allow blood to flow in one direction around the body, preventing backflow of blood into the chamber from which it was pumped. In simple terms, blood returns from the body via veins into the right (R) atrium and this is then pumped into the larger R ventricle, before contraction of the R ventricle pumps blood back through the lungs to be oxygenated. The oxygenated blood then returns into the left (L) atrium before moving into the L ventricle where strong muscular contractions pump it out around the rest of the body to deliver the oxygen and collect the waste products generated by cells, which is crucial to survive.
Valves are located between the atria and the ventricles, and also where the blood exits from the ventricles into the arteries. These are:
- Mitral valve — situated between the L atrium and the L ventricle
- Aortic valve — situated between the L ventricle and the Aorta
- Tricuspid valve — situated between the R atrium and the R ventricle
- Pulmonary valve — situated between the R ventricle and the pulmonary artery
The role of the valve is to allow the blood to flow through but prevent the backflow into the chamber from where it came. When a valve doesn’t function properly and blood is able to escape back through the valvular leaflets, turbulence occurs creating an audible murmur.

Murmurs are characterised according to the location in the heart, their loudness, and the timing/duration in the cardiac cycle that the murmur is heard. Location is determined by listening to the murmur and detecting the point it is heard the loudest, commonly called the “point of maximum intensity (PMI)”. The mitral, the aortic and the pulmonary valve sounds are all heard best on the left side of the chest, whereas the tricuspid valve is better detected on the right side. Although the PMI is characteristically heard in a certain location for each valve, this area does not correlate with the anatomical site of the valve but the site where the vibration caused by the turbulence is loudest.
The intensity or loudness of the murmur is graded from 1 to 6 with a Grade 1 murmur barely audible and a Grade 6 murmur loud enough to hear with a stethoscope that is raised off the skin. Although many correlate the intensity of the murmur with the severity of the murmur — the louder murmurs being the more significant ones — this isn’t always the case as occasionally some severe murmurs can produce quiet musical sounds.
The timing and duration of the murmur is used to classify its type and relates to whether the heart ventricles are contracting (systolic) or dilating (diastolic). Most murmurs are systolic murmurs, and these are heard between the “lub” and the “dub” sound most of us associate with listening to a heartbeat. There are murmurs that are heard throughout the whole systolic period and others that are only heard for a short phase during systole. Diastolic murmurs are heard after the “lub-dub” beat and are far less common. On a rare occasion, a murmur can be heard continuously throughout the entire cardiac cycle.
Physiologic Flow Murmurs (PFM) are created in normal horses because of the large heart size and the large amount of blood that is pumped out when the ventricles contract, causing large volumes of blood to flow out into the aorta and pulmonary artery. These murmurs are often heard early in systole and are very short in their duration as they arise when the aortic and pulmonary arteries initially open as the ventricles collapse and blood is ejected into the large blood vessels (similar to the gates on a dam being opened and water surging through). PFM can also be heard early in diastole and may be due to the initial flow of blood back into the ventricles from the atria as the ventricles relax.
Mitral Regurgitation (MR) is perhaps the most common murmur auscultated in the horse and this can be caused by mitral valve prolapse, thickening of the valve, malformation of the valve or rupture of the connective tissue that supports the valve. Many horses with MR can continue to compete successfully as an athlete but this will be dictated by the severity of the valve damage and highlights the importance of assessing the valve with cardiac ultrasound.
Aortic Regurgitation (AR) occurs more commonly in adult horses and is often associated with degeneration of the valve. In mild cases, athletic performance is not affected but as the horse ages, the AR is likely to deteriorate and annual check-ups to monitor the horse’s heart are recommended.
Tricuspid Regurgitation is not an uncommon finding in thoroughbred racehorses with no effect on performance detected. Usually there is no pathology of the valve causing the blood to flow back into the R ventricle, but instead the blood is able to flow back through the valve because the right ventricle has become enlarged simply by exercise producing normal muscle enlargement in that side of the heart. There are however, some instances where the valve can be deformed or the connective tissue supporting the valve can rupture, so it cannot be assumed that all cases of TR are irrelevant to the health of the horse.
Pulmonary Valve disorders are rare and are more likely to be associated with other cardiac abnormalities.
Endocarditis is a bacterial infection of the endocardium or inner lining of the heart, but mainly presents as a bacterial growth on the valve referred to as a vegetative lesion. This vegetative growth affects the valve’s function and reduces the valve’s ability to close and stop backflow of blood into the chamber. The murmur detected on auscultation will depend on where the growth is located (which valve) and the size of the vegetative growth. It is usually diagnosed using an echocardiogram, as the growth can be visualised directly. It can occur in foals that have had septicaemia but is also seen in mid- to old-age horses without any cause identified. In older horses, the aortic valve is more commonly affected, but cases can occur on both the mitral and tricuspid valves. Vegetative lesions on the tricuspid valve are usually the result of an infection in the jugular vein from an intravenous needle or catheter.
A “hole in the heart” will cause a murmur that is detected on cardiac auscultation and is the most common congenital heart abnormality that can occur. A hole can occur between the two atria or between the two ventricles, however, it occurs more frequently between the left and right ventricle. A hole between the ventricles is referred to as a Ventricular Septal Defect (VSD) and forms during foetal development. The size of the hole determines the effect the defect will have on athletic performance and life expectancy, with small defects having minimal effect on performance or life expectancy and much larger holes unable to support any athletic pursuits and result in a premature death. These holes can also be associated with other congenital defects in the heart, so if a murmur is suggestive of a VSD, a thorough cardiac evaluation is recommended.
Patent Ductus Arteriosis (PDA) is a rare cause of cardiac murmur when detected after a couple of days of age and produces what has been described as a machinery murmur (a continuous murmur that changes intensity throughout the cardiac cycle). A PDA can be heard in healthy day-old foals sometimes, but its persistence past a day or two is pathological and signals the existence of a complex congenital defect that is usually incompatible with life.
There are several other murmurs that can be generated in the heart and most will require a full cardiac workup to identify the origin and the significance of them. Unfortunately, with the possible exception of some bacterial infections on the valves, most pathological murmurs cannot be cured, and the aim is to differentiate the murmurs that are compatible with athletic performance from those that affect performance but are compatible with life and those that are not compatible with life. EQ
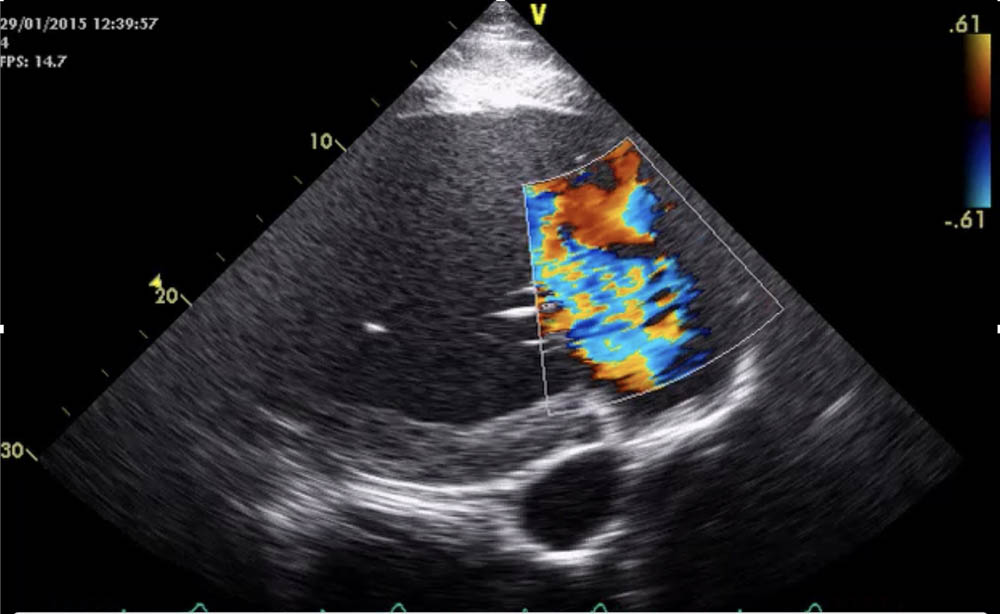
Heart imaging courtesy of Laura Nath: BVSc (Hons), MVSc, CertEM, FANZCVS. Registered specialist in Equine Medicine. PhD candidate University of Adelaide.
YOU MIGHT ALSO LIKE TO READ BY DR MAXINE BRAIN:
Matters of the Heart – Equestrian Life, January 2023
Umbilical Concerns in Foals – Equestrian Life, December 2022
Retained Foetal Membranes – Equestrian Life, October 2022
Preparing for Laminitis – Equestrian Life, September 2022
Working Together for Best Outcomes – Equestrian Life, August 2022
What Constitutes an Emergency – Equestrian Life, July 2022
Peri-Tarsal Cellulitis Calls for Quick Action – Equestrian Life, June 2022
Sinusitis: Not To Be Sneezed At – Equestrian Life, May 2022
Japanese Encephalitis: No Cause For Alarm – Equestrian Life, April 2022
Hernia Learning Curve – Equestrian Life, March 2022
Osteochondromas: Benign But Irritating – Equestrian Life, February 2022
Don’t Forget the Water – Equestrian Life, January 2022
Understanding Anaesthesia – Equestrian Life, December 2021
A Quick Guide to Castration – Equestrian Life, November 2021
Caring for Mammary Glands – Equestrian Life, October 2021
Sepsis In Foals – Equestrian Life, September 2021
Understanding Tendon Sheath Inflammation – Equestrian Life, August 2021
The Mystery of Equine Shivers – Equestrian Life, July 2021
Heads up for the Big Chill – Equestrian Life, June 2021
The Ridden Horse Pain Ethogram – Equestrian Life, May 2021
The Benefits of Genetic Testing – Equestrian Life, April 2021
Heavy Metal Toxicities – Equestrian Life, March 2021
Euthanasia, the Toughest Decision – Equestrian Life, February 2021
How to Beat Heat Stress – Equestrian Life, January 2021
Medicinal Cannabis for Horses – Equestrian Life, December 2020
Foal Diarrhoea Part 2: Infectious Diarrhoea – Equestrian Life, November 2020
Foal Diarrhoea (Don’t Panic!) – Equestrian Life, October 2020
Urticaria Calls For Detective Work – Equestrian Life, September 2020
Winter’s Scourge, The Foot Abscess – Equestrian Life, August 2020
Core Strengthening & Balance Exercises – Equestrian Life, July 2020
The Principles of Rehabilitation – Equestrian Life, June 2020
When is Old, Too Old? – Equestrian Life, May 2020